A guide forusers & professionals
This booklet is designed to provide information about the use of anabolic steroids and some of the other drugs that are used in conjunction with them. We have tried to keep the booklet free from technical jargon but on occasions it has proven necessary to include some medical, chemical or biological terminology. I hope that this will not prevent the information being accessible to all readers. The booklet is not intended to encourage anyone to use these drugs but provides basic information about how they work, how they are used and the possible consequences of using them.
If you feel you would like more information then you could read Anabolic Steroids and other Performance Enhancing Drugs by Pat Lenehan (Taylor and Francis, 2003)
Anabolic Steroids

A guide for
users & professionals
Contents
Formation of Testosterone 8
How Steroids Work (illustration) 10
Section 1 How Steroids are Used 13
Side Effects of Anabolic Steroid Use (illustration) 20
Women and Side Effects 26
Human Growth Hormone 28
Human Chorionic Gonadotrophin (HCG) 31
Nandrolone Decanoate 36
Methandrostenolone 37
Oxandrolone 38
Oxymetholone 38
Stanozolol 39
Sustanon 250 40
Testosterone Enanthate 40
Testosterone Cypionate 41
Methenolone Acetate 42
Section 5 Intramuscular Injections for Anabolic Steroids 45
Drawing up From an Ampoule or Vial 48
Injection 52
Complications of Poor Injecting Techniques 54
Introduction
Anabolic steroids are basically synthetic versions of the male hormone testosterone.
They have two main effects on the human body; an anabolic, or muscle building, effect and an androgenic, or masculinising, effect. The realisation that increases in weight and strength can be achieved by their use led to a widespread use of steroids in sport and today there is hardly a strength sport in which anabolic steroids have not been used. Their availability from illicit sources has made them readily available and now they are so widespread that they can be found in most areas where serious training is being pursued. Nowadays the biggest group of users are probably non-competitive users whose reason for use is purely cosmetic.
Anabolic steroids are not the same as corticosteroids (such as cortisone and prednisolone) which are medically prescribed to treat asthma and skin disorders or as anti-inflammatories. Cortico steroids have no muscle building or masculinising effects. Whenever the term steroids is used in this booklet it refers to anabolic steroids.
“…the biggest group of users are probably non-competitive users whose reason for use is purely cosmetic…”
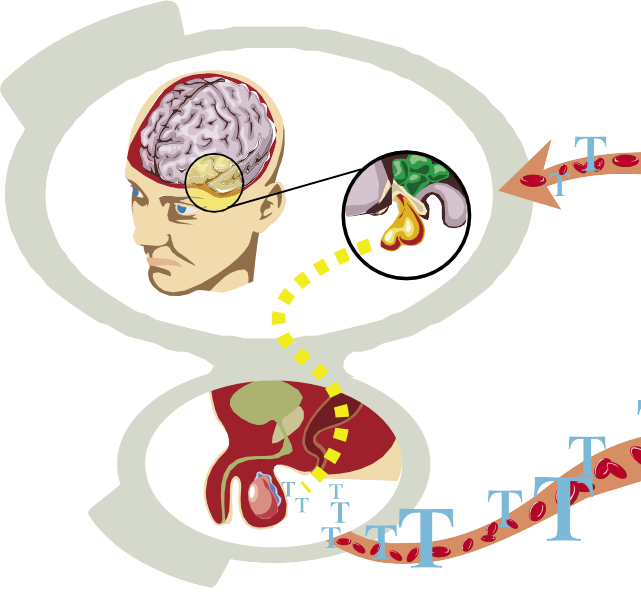
Formation of Testosterone Testosterone is secreted by the testes, the adrenal gland, the ovaries and the placenta. It is synthesised from cholesterol by a complicated series of steps within the steroid secreting cells. The stimulus to form testosterone comes initially from the hypothalamus; an area of the brain where several hormones are developed which relate to the function of other glands.
The hypothalamus releases Gonadotrophin Releasing Hormone (gnrh) which is delivered to the pituitary gland by a special group of veins known as the portal system. Once delivered there, it causes the pituitary gland to form Luteinising Hormone (lh) that is released into the blood stream. It is then transported to the testis where the Leydig cells form testosterone from the cholesterol that has been stored there for that purpose. Once the testosterone is formed it is secreted into the blood stream where most of it is bound to protein and is transported in the bound state throughout the body. It is only the free testosterone that is capable of being biologically active. Only 1 to 3% of the total testosterone in the blood is able to interact with receptors in the tissue targeted for its use.
There is a feed back mechanism to the pituitary, which controls the rate of synthesis of the hormone. This feedback mechanism is controlled by the blood level of testosterone. As testosterone levels are increased, the secretion of gnrh and as a result, Luteinising Hormone, is reduced and may be totally inhibited. This leads to a reduction in production of the hormone and maintains equilibrium. When the blood level of testosterone falls, the reverse occurs and pituitary secretion is increased to restore balance.
The total daily production of testosterone in a male is about 7 mgs per day.
Method of Action
The free testosterone in the serum is the only active part of the hormone. This amount represents about 2% of the total hormone present in the circulation and its half-life, that is, the time taken to destroy half of the substance, is 10 minutes.
When testosterone is brought into the cell it is firstly converted to 5 alpha di-hydrotestosterone (DHT) and then the work of the cell can proceed. The next step is the binding of the hormone with an androgen receptor (AR) in the cell to form a complex, which can be transported into the nucleus where the important reactions take place to build muscle. There are not separate receptors for oral and injectable steroids or for different esters. The actual protein formed depends upon the cell in which the reaction is occurring. Thus, irrespective of which anabolic steroid is used, a muscle cell can only form muscle protein.
Once a complex has been formed, the resultant substance is then transported into the nucleus where it activates genes to produce the appropriate protein. This is then released into the cytoplasm of the cell to perform its action. The characteristics of the particular cell determine the response. Muscle cells can only produce muscle protein, just as prostate cells can only make prostate protein as a result of steroid use. Differences in the various drugs are due to the effect of excess material being free in the blood and affecting other organs such as the brain, where it may cause altered emotional effects. The receptor numbers in the cell are limited and once saturated they cannot combine with extra material, thus limiting the anabolic effect of large doses or extended courses. This is referred to as the refractory phase. As muscle cells hypertrophy, the receptor numbers increase slightly but this is not enough to require large amounts or extended courses for saturation.
There is evidence that some steroids may bind to more than one receptor. The most frequent one is the glucocorticoid receptor and there, the steroid will replace the cortisone like substance usually present. Corticosteroids have the effect of breaking down tissue and any reduction in this activity is continued on page 12
How Steroids Work
![]()
![]()
![]()
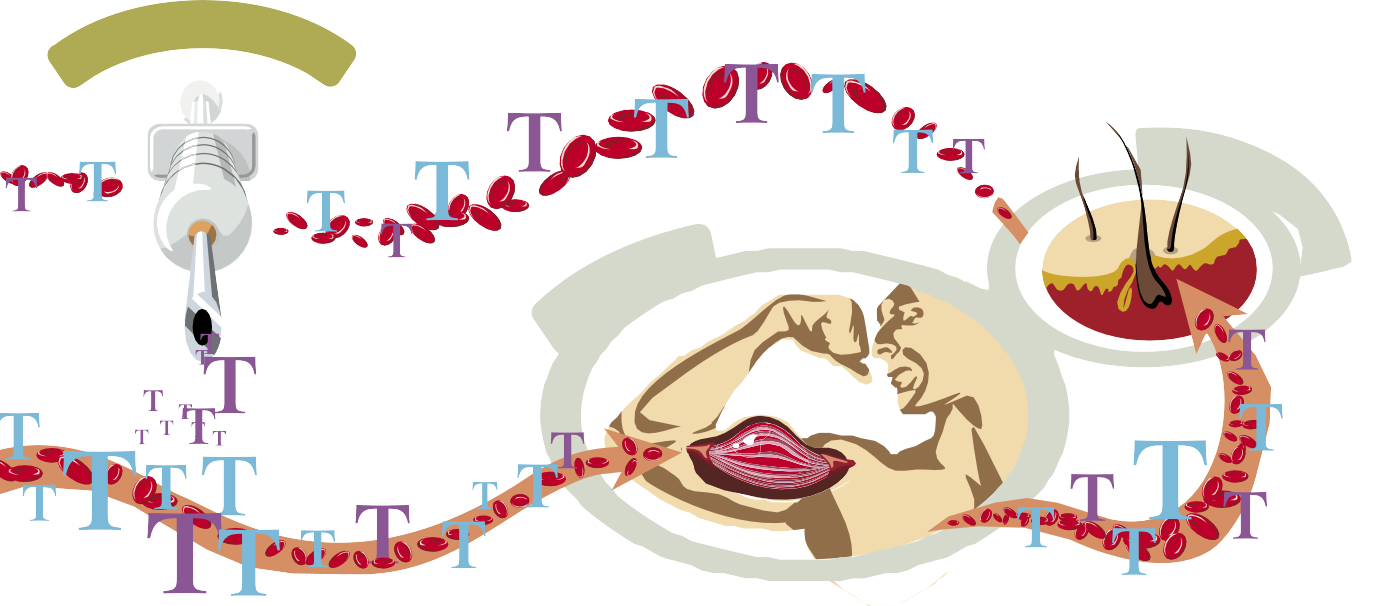
- beneficial in building up the body but, when the steroid course is finished, the reverse action occurs and there is an increase in catabolism as a result of the corticosteroids being taken up by the receptors again. This may be one reason for the weight loss that occurs in some users at the end of the course.
Once the steroid has been metabolised in the nucleus, it is taken from the cell and degraded in the liver. From here it is excreted in the bile or the urine. The actual excretion products vary from one androgen to another and it is these products that are detected in sports drug testing. Testosterone is rapidly destroyed by the liver, making the substance useless as an oral anabolic agent unless it is bound with some other radical. For oral use of testosterone, a chemical group is added to the molecule to allow absorption from the stomach, enabling the testosterone to bypass the liver. This increases the duration of the action of testosterone by allowing more of the active substance to reach the muscle cells.
Testosterone is important in the development of the sexual differentiation and the development of the external genitalia before birth. These are the androgenic effects of testosterone. At puberty it leads to the growth of masculine characteristics such as increased muscularity, deepening of the voice, development of the beard and secondary sexual features. With the increase in testosterone secretion at puberty, there is a growth spurt with lengthening of the long bones and eventually closure of the end of these bones, epiphyses. It also increases the secretion of the sebaceous glands. The other major effect of testosterone is anabolic and the increased muscle growth that this produces. This is the greatest attraction for athletes.
To try and develop an ideal anabolic agent without androgenic effects many changes have been made to the structure of the molecule. This search has gone on for many years without the desired result. To date, all steroids have anabolic and androgenic actions.
A review of the chemical structure of the common anabolic steroids shows how similar they all are.
Section 1: How Steroids are Used
 If anyone is considering using steroids it is essential to have an understanding of the potential benefits and side effects of using them.
If anyone is considering using steroids it is essential to have an understanding of the potential benefits and side effects of using them.
 It is important that the user should not be unrealistic in expectations and realise that large and permanent gains cannot be made in one course. Every athlete is different, in his or her genetic make-up. Training, diet regulation, illness and stress determine the response to steroids.
It is important that the user should not be unrealistic in expectations and realise that large and permanent gains cannot be made in one course. Every athlete is different, in his or her genetic make-up. Training, diet regulation, illness and stress determine the response to steroids.
Steroids are generally used in cycles and are often taken in stacks. Stacking refers to the practice of taking several drugs simultaneously. This is common among anabolic steroid users and can also involve the use of drugs other than steroids. Cycling refers to the pattern of steroid use where drugs are taken in cycles of a period of weeks followed by a drug free period.
A major factor is the number and distribution of androgen receptors in the muscle. There is no universal pattern of distribution of the receptors but the greater concentration is generally in the upper body, leading to a greater response in the arms than the legs in most, but not all individuals. The number increases slightly, as the muscle grows and this may be a reason for some athletes having larger gains with their later course.
“Training, diet regulation, illness and stress determine the response to steroids.”
A weight-training programme will lead to increased strength and an increase in muscle mass. Steroid use should not be considered until the athlete has plateaued, that is, there is no more increase in weight and strength in spite of continued heavy training before using steroids.
The importance of diet cannot be overemphasised and must contain sufficient carbohydrate food to support a training programme. The muscle needs protein to grow but it cannot work efficiently without the fuel and this is best provided by carbohydrate foods. Carbohydrate also attracts water into the muscle cell and this results in an increase in the bulk of the muscle.
What steroid?
All steroids produce the same result at the end of a course. They stimulate the cell nucleus to produce the protein characteristic of the cell. In the case of muscle cells, that will be muscle protein. This is the desired result of using the steroid. There is no doubt that there are differences in the effects of the different steroids when taken in a single dose and monitored over some weeks. With the testosterone preparations, there are differences in the rate at which they are taken up from the injection site.
These differences refer to one dose but steroids are not used as a single dose but rather as a series of doses over a period of time and this invalidates many of the conclusions based on duration of effect when those assumptions are based on a single dose format.
There is a question of whether to use oral or injectable drugs. There is no difference in the overall effects if the athlete trains correctly, the route of administration is not the most important factor.
There are variations in the rate of uptake of different steroids by the steroid receptors. Once again, this is not an important factor in choosing a steroid as they are used over a period and any gain that one may have on the first dose is insignificant when a course lasting several weeks is considered. It is the final result that is important.
For a second or later course of a drug, there is no reason why the same anabolic steroid cannot be used. The body does not develop tolerance and results can be achieved with the same steroid, providing that the training programme and diet are adequate.
How much to use?
There has been no scientific research performed to find out the effect of a specific amount of steroid on a weight training programme. The information available is related to steroid use in medicine, and there, the expectations are different from those seen in training for weight gain.
It is important to recognize that if a gain is made with a large dose of steroids, it is not necessarily true that the dose was the right one. Many of the large doses produce the same result as smaller doses with the excess steroid being spread around the body to other areas where side effects are produced before the material is destroyed in the liver. There is a limit to the amount that the androgen receptors and the cell nuclei can take up and once they are full, they cannot handle any more steroids at that time.
To double the effect in animals takes about 10 times the original dose but in humans this would produce excessive side effects. There must be a dose at which no significant benefit accrues but by continually increasing the dose and the variety of steroids used, one cannot constantly improve the results obtained. The most important factor in gaining weight is the combination of correct diet and an adequate training programme.
Increasing a dose may not increase the muscle building effect but it will increase the chances of, extent of and types of side effects experienced.
Length of courses?
Long continued courses of anabolic steroid do not lead to continuing weight and strength gain. There is in some athletes, an immediate response to anabolic steroids and others take up to 3 weeks to show any development. There is a continuing growth pattern generally lasting for some 6 to 8 weeks. They plateau at this level and further steroid use produces little or no benefit.
Once the steroid receptors are full and probably fatigued, no further gain is to be expected. It is advisable to restrict courses to no more than 6 to 8 weeks. If muscle gains are not apparent in that time, the cause is generally not insufficient steroids, but a problem with the training regime or the diet.
How often to use steroids?
This is a difficult question to answer. It is important to have goals when using steroids as this will make it possible to evaluate progress. If progress is not being made then it may be that the goals may be unrealistic. A strength gain of around 5% over 6 to 8 weeks is good in an early course, although it is often difficult to estimate strength gains with any degree of accuracy. In future courses it is more difficult to attain these types of gains as people approach the maximum for their body as it is not possible to continuously increase strength. A slightly lower gain exists with muscle mass where 3% might be considered a good result. Once again it is not possible to continue the same rate of gain with subsequent courses.
Most people lose weight after a course of anabolic steroids has finished. Many users find it difficult to maintain the high level of effort required for maintenance and as a result, lose weight. There is, in some athletes, a retention of water during the course and when the steroids are stopped, this water is lost and the scales demonstrate a weight loss over a few weeks.
The decision to use another course should be carefully assessed and a new goal set. The quicker a new course is started, the less the gain to be expected, as the benefits of the previous course are still evident and receptor recovery has not occurred. It is wise, in a person who has maintained a heavy training programme, that the interval between courses be at least as long as the duration of the course just completed. This allows a reasonable time for the body to recover from the effects of the prior course.
Section 2: Side Effects
ll drugs have the potential to cause side effects and anabolic steroids are no exception to this. The cause of the side effects may be due to an individual having an unusual reaction to the drug or it may be related to using too much. It must be remembered that what one person can use safely, may be dangerous to another. As a rule of thumb the more steroids used the greater the risk of side effects and the more serious they are likely to be. However, there are also instances of people reacting adversely to low doses of steroids. There may also be evidence of taking other drugs, which can exaggerate the steroid effects.
Potential effects can be reduced or avoided by being aware of the problems. Many but not all of the side effects are of a temporary nature and will resolve within some weeks of ceasing the drugs. Knowledge of the side effects will allow you to recognise early signs and thus reduce the overall risks.

“…the more steroids used the greater the risk of side effects and the more serious they are likely to be…”
Skin
Acne is a common side effect of steroid use and is commonly seen on the back. The larger the amount of steroid used, the greater the likelihood that acne will develop. To help to minimize the risk, it is helpful to ensure that the skin is kept clean and oily substances avoided. The acne develops slowly and should be watched for by those who believe that they may be susceptible to the problem. Once it shows signs of developing, all steroids should be discontinued. The acne should abate over a period of 3 to 4 weeks. If this does not occur, medical advice should be sought, being sure to tell your physician that you have used steroids.
Some users develop a fine follicular rash over the trunk after some 3 or 4 weeks use of the drug. This is not acne but a follicular dermatitis, which should disappear when steroids are stopped.
Breasts
Gynaecomastia is a condition in which the mammary glands, or breasts, enlarge and become sore and tender to touch. It is due to the chemical change in testosterone brought about by a process called aromatisation, when the male hormone is converted to a form of oestrogen, the female sex hormone.
There is initially a sore feeling in the breast. A skin ridge appears on the outer side of the areola together with a halo appearance around the area but no swelling. As the course continues, a swelling develops and it becomes tender. Fatty tissue builds up around the area and the breast becomes prominent. At times there may be a secretion of fluid from the nipple when it is squeezed. Steroids should be stopped. If recovery does not occur by the end of 2 months, surgery should be considered. Other causes of gynaecomastia that may need to be considered are the use of medications such as Tagamet, a treatment for gastric problems, HCG and spironolactone. Some body builders use this latter drug to reduce body fluid. Occasionally boys in the post-pubertal phase develop breast enlargement due to endocrine imbalance totally unrelated to steroids.
Heart
There have been cases of people who have used anabolic steroids suffering from a heart attack and dying. This group has shown evidence of coronary artery blockage that was responsible for their deaths. It is therefore important for anyone considering the use of anabolic steroids to have a medical check up before starting to use steroids.
Raised total cholesterol and low levels of High Density Lipoprotein Cholesterol (hdl) are known to predispose to heart disease and should be measured before starting steroid use. Total Cholesterol is little affected by steroids but the drug sometimes lowers hdl (good cholesterol) and increases Low Density Lipoproteins ldl (bad cholesterol). The lowering of hdl levels is due to the effect of the steroid on the liver and this applies to injectable as well as oral drugs.
Cardiomyopathy, a disease of heart muscle, has been recorded in anabolic steroid users. It presents usually as a form of weakness and breathlessness and needs medical advice for its evaluation.
Hypertension, or high blood pressure, has been reported with steroids but there is little evidence to support a cause and effect mechanism. Any high blood pressure might not be caused as a direct result of steroid use but may be associated with other side effects such as heart liver or kidney problems.
If there are any symptoms that suggest heart disease, a medical opinion should be sought immediately. The principal complaints might be shortness of breath with or without effort, chest discomfort and feelings of faintness.
Fluid Retention
There are some people who retain excess fluid when on a course of steroids and feel bloated. This is most easily seen in the face and around the neck region. It generally disappears within a few days of stopping the drug. Should this not happen, medical advice should be sought, as there are other causes of water retention. As a consequence of the water loss, there will be a loss of weight in that period, but this does not indicate a loss of muscle mass as this continued on page 22
Side Effects of Anabolic Steroid Use
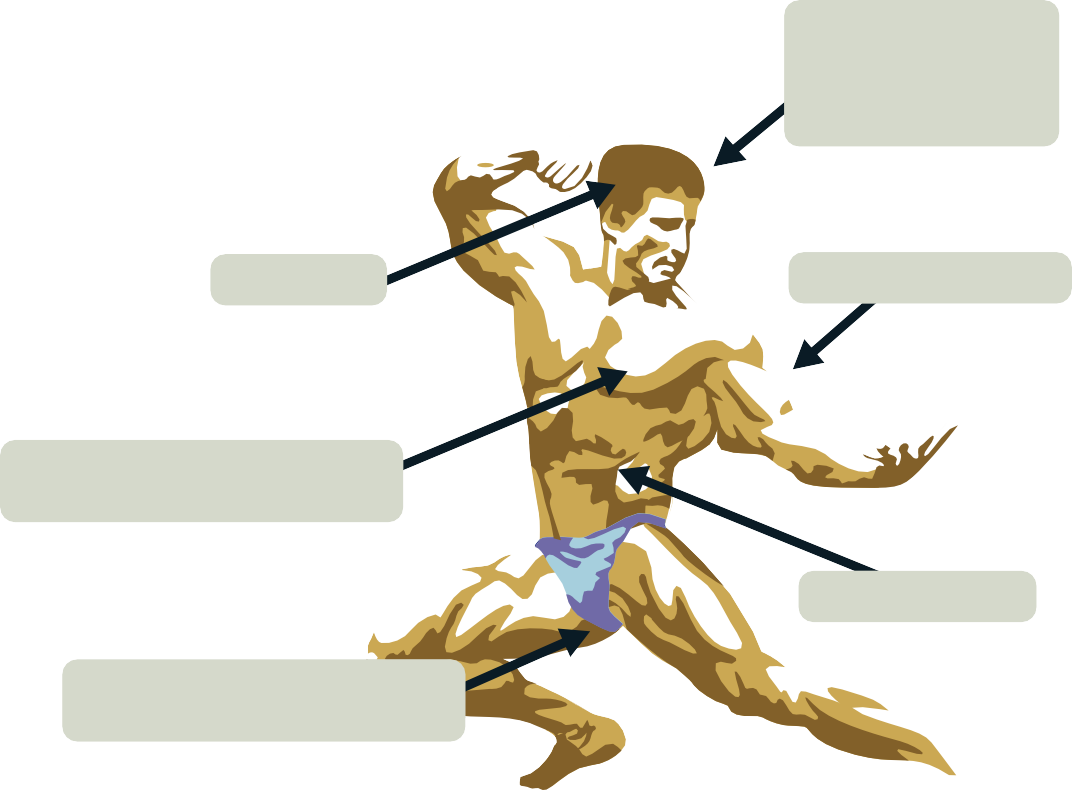
AGGRESSION LIBIDO CHANGES INSOMNIA
HAIR LOSS TENDON DAMAGE
GYNAECOMASTIA
(Breast development or enlargement)
LIVER DAMAGE
SHRINKING TESTICLES PROSTATE ENLARGEMENT
FACIAL HAIR ACNE
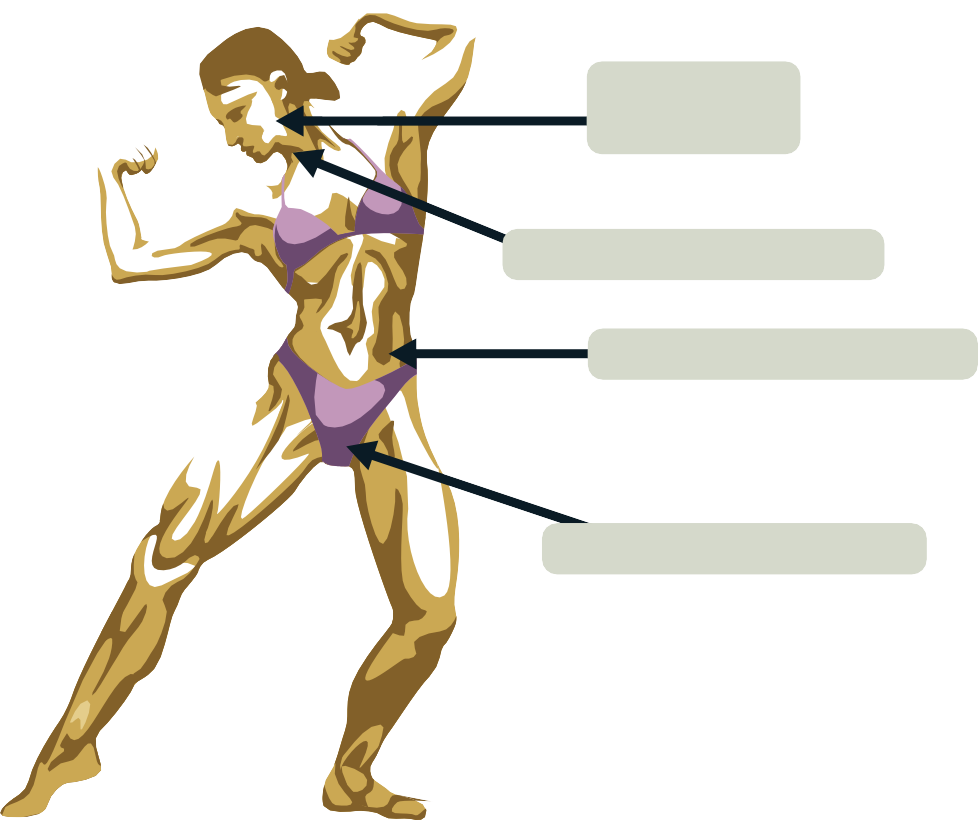
DEEPENING OF THE VOICE
ROUGHENING OF THE SKIN
CLITORAL ENLARGEMENT
fluid is in the space between muscle fibres and not inside the fibres. This is not an indication to increase the amount of steroid used in the next course, as a lack of steroid is not the cause of the condition.
More steroid will accumulate more fluid and lead to a greater loss of weight and size at the end of the course. It does not occur in every user to a degree where it is obvious, but many athletes report a sudden loss of weight after the first few weeks of finishing a course and this is almost certainly due to water loss and not loss of muscle mass.
Aggression
Aggression can take many forms:
-
- Physical assault
- Indirect hostility
- Irritability
- Negativism
- Resentment
- Suspicion
- Verbal hostility
It is important that all anabolic steroid users study their own reactions to the drugs. When it becomes apparent that any of the above states is becoming evident, then the user should stop. The user should take time to assess his position. Not all drugs cause the same feelings, as there are minor chemical differences between the drugs that affect their metabolism in the emotional centres of the brain. Large doses are not only wasteful but also lead to more problems with the emotional symptoms.
Liver Changes
Many steroids cause changes in liver function as shown by alterations in the liver function tests. This is most frequently seen with the oral preparations that are alkylated at the C-17 position. There have been cases of jaundice reported when steroids have been used but these have often been in patients who used unusually large doses or who were suffering from medical diseases. Peliosis hepatica, a condition in which there are blood filled sacs in the liver has been found in people using steroids. Liver tumours have been noted in people who used anabolic steroids. It is difficult to prove cause and effect, but in some people the tumours have decreased in size after withdrawal of the steroid, suggesting that the drug may stimulate tumour growth rather than cause it.
Sexual Disturbance
Anabolic steroids may cause a disturbance in sexual function. The use of anabolic steroids depresses the formation of the pituitary hormones that affect the function of the testis. Follicle Stimulating Hormone (fsh) is responsible for the formation of sperm and Luteinising Hormone (lh) stimulates the formation of testosterone. Both of these functions are suppressed, at least in part, by anabolic steroids and it is inevitable that the size of the testis will be effected to some degree with their use. This decrease may not be noticed by the individual but is present nevertheless. The degree of decrease in size of the testes varies among users and at times can be quite obvious.
The prolonged use of anabolic steroids will cause a greater loss of size than a short course and the higher the dose, the more likely it is that the testes will decrease in size to a notable degree. Following the cessation of the drug, the testes usually return to their normal size, but in those who have used long or high dose courses it is not uncommon for the changes to persist for many months even up to a year or two. If the reduction of the testes persists, medical advice is needed to restore the bulk of the testes and even then, the recovery may be prolonged. The reduction in Follicule Stimulating Hormone decreases the amount of sperm and decreases the likelihood of pregnancy but this is not a guarantee of contraception. Extended courses may lead to a temporary sterility lasting several years possibly even permanently.
Steroids have an effect on libido. This varies widely from over stimulation to a total loss of libido. When the latter occurs, the athlete should cease the course and wait for the expected return of the sex drive.
This does not always happen as the sexual act is a very complex act and there are many causes of impotence. The cause of the loss of libido is not a lack of testosterone. It is due in most cases to outside influences and a few shots of steroids will not fix it but make it worse. In women there is sometimes an increase in libido when using the drug but this will return to normal on cessation.
Bleeding
Anabolic steroids cause a lengthening of the bleeding time and this can lead to bleeding from the nose, mouth or other orifice. If this occurs and does not settle quickly, or is recurrent, a doctor should be consulted to ensure that there is no serious clotting deficiency that could put a user in a precarious position as a result of a sudden bleed after little trauma such as forcibly blowing one’s nose. It goes without saying that the doctor should be told of the history of steroid use. There is evidence of some athletes suffering a stroke when using steroids due to clot formation, the opposite of bleeding. The clotting mechanisms are very complex and these events are usually associated with large doses. To date the research into this area has not fully explained the different results of steroids on the clotting mechanisms. Similar events have been described in women using the contraceptive pill.
Hair Loss
Balding is part of the genetic make up of many males. In any male who has a predisposition to it the use of steroids may speed up the process. It should be noted that a hair loss might occur in men who have never used a steroid.
Insomnia
If it is difficult to sleep when using steroids the best approach is to cease the drug. Using sleeping tablets will not cure the problem and may have a hangover like effect.
Tendon Damage
Anabolic steroids strengthen muscle and not tendon and there is an increased likelihood of tendon rupture in the users. The event is sudden and demands immediate attention. The most common tendon affected is the biceps tendon and the tear may be partial or complete. It is important that there be no further use of the arm until the problem has been fully evaluated by a doctor. The other frequent site for muscle rupture is in the quadriceps group.
Young People
Anabolic steroids have been reported to be associated with stunting of growth in adolescents. The steroids may lead to premature closure of the epiphyses of the bone. This is the growing part of the bone and once union at that site has occurred, no further increase in height is possible. This will decrease the future benefits of steroids for those interested in appearance or body building competitions. Once this has happened there is no method by which it can be reversed.
Prostate Gland
Studies have shown that the prostate gland increases in size during a course of anabolic steroids and it will decrease after the course. This is of particular interest to the older male who uses these substances as this age group in particular is susceptible to urinary blockage due to swelling of the gland. If there is a difficulty in passing urine in the form of trouble in starting the flow, anabolic steroids should be ceased and medical attention is needed. It is important to establish the correct diagnosis early to enable simple curative measures to be undertaken. Even the young person needs to consider this side effect when faced by urinary problems.
Infections
The commonest infection during the course of steroid use is the one due to lack of sterility in the technique. It can be avoided by using a new syringe and needle for each injection and making sure that the hands are washed before any preparation is done. The infection will show up as an abscess at the site of injection.
This may be superficial or deep – the latter may take several days to develop. Once there is a suspicion of an abscess formation medical help is needed immediately.
Anabolic steroids have also been known to have an effect on the immune system and some users have been known to complain of having more colds when using steroids.
The other source of infection comes from sharing injecting equipment. This is one way HIV and Hepatitis are spread.
Women and Side Effects Anabolic steroids can produce unwelcome side effects in a female user and it is very important that the initial signs be recognized early. The development of deepening of the voice is a sign of virilisation. Once this has been detected, the drug must be stopped to allow some degree of recovery. The recovery may not be complete in all cases. Any hoarseness that remains after 3 months is likely to be permanent.
Clitoral enlargement is not an obvious disability in the early stages and is often ignored for that reason.
Skin changes are obvious in many women. Change in texture of the skin is the first abnormality seen. The development of facial hair is of two types, namely, a fine downy hair over the face that will disappear on stopping the drug, and a darker hair in the beard area. This latter hair is likely to remain.
Irregularity of periods or, at times, a total cessation of them, may be due to steroids. As courses should only be of 6 weeks duration at the most, it is often hard to be sure that the absence of a period is due to steroid use. Courses of longer duration are more likely to cause longer periods of amenorrhea and so require a longer spell of steriod abstinence. It is important that if another course is contemplated, a resumption of periods must be awaited before starting the next course. Pregnancy is the commonest reason for missed periods and needs to be eliminated before any other treatment is considered. Once this has been done, any glandular abnormality should be investigated.
Section 3: Other Drugs
here are a large number of drugs such as growth hormone and diuretics used in association with anabolic steroids for

Tmany reasons including water loss, strength gain and increased muscle mass. However, the most consistent characteristic of these drugs is the absence of scientific data to support their use.
Research has not been conducted on their effects during exercise and there may be unexpected adverse results with their use.
Most of the known information on the use of these substances in exercise is anecdotal and based on a single case. Their use is generally based on some action known to occur in a biochemical pathway in the ill person and it is assumed the same effect will occur in the well person. It is important that the action of a drug is understood before it is used as this will help to prevent unnecessary adverse side effects.
“…the most consistent characteristic of these (other) drugs is the absence of scientific data to support their use…”
Human Growth Hormone Human Growth Hormone (gh) is formed in the pituitary gland as a result of the stimulus of a hormone released from the hypothalamus, Growth Hormone Releasing Hormone. This is transported to the pituitary gland which then releases gh into the circulation. There is another hormone, Somatostatin, released by the hypothalamus, which reduces the amount of gh formed and these two hormones control the level of gh in the circulation. The hormone is produced on an intermittent basis and its levels in the circulation fluctuate during the day. As it is not bound to protein, once formed, the cells must use it.
Gh is now made commercially and produced by genetic engineering and has specific medical
uses. Previously it had been extracted from human cadavers but this has a risk of causing Crakob- Jeutzfeld Disease, a disease of the central nervous system. The production of gh leads to the release of Somatomedin, principally Insulin Like Growth Factor- 1 (igf-1) from the liver and other tissues. Illness, psychological stresses and exercise can also affect gh formation.
A major action of gh is on glucose metabolism and sodium balance. Gh causes hyperinsulinaemia, a high insulin level, and impairs the ability of insulin to suppress the formation of glucose in the liver.
This increases the likelihood of developing diabetes. Another action of gh is to increase nitrogen retention in the body and build up the protein in tissues. To do this, it is essential to consume an adequate calorie supply. This action affects many tissues. Prior to closure of the epiphysis, or growing part of the bone, gh stimulates the lengthening process, but after closure, it causes the bone to broaden and thicken up. Gh leads to enlargement of the skeletal muscle mass, the attached tendons, the liver, lymph glands and the thymus gland. It diminishes the level of adipose (fat) tissue and has been used in clinics over the world to reduce body fat in the older population.
The attraction of gh to athletes is that it causes increased muscle and tendon strength, making rupture less likely. The major side effect of gh is the overgrowth of the bone. This is most apparent in the forehead region when overhanging brows are seen. There is also the tendency to develop diabetes when using gh and it is wise to test the urine regularly. As a result of the widespread effects of gh, there may be the development of cardiomegaly, an increase in the size of the heart. In this instance having a bigger heart is not an advantage to the user and is likely to lead to heart failure.
Insulin
Insulin causes changes in the metabolism of carbohydrate and fats in particular. Insulin is important in the human body as it regulates the level of blood sugar, which fluctuates with food intake. It also promotes the uptake of amino acids by the cell and increases protein synthesis. It is impossible to dissociate these actions and while there may be some gain in muscle, there will also be an increase in fat levels.
There are risks in the use of insulin. The most likely problem is hypoglycaemia, a lowering of the blood sugar to a level where there may be an abrupt loss of consciousness and the individual collapses. Using this substance is particularly dangerous for a person who may drive a car, work near machinery or at heights.
Hypoglycaemia is recognised by a feeling of faintness, sweating and a shaky sensation. At times there is an onset of nervousness for no apparent reason. There is a sensation of confusion and uncertainty. At this time, some food should be taken to prevent further symptoms. If the diagnosis is wrong, no harm is done, but if a warning is ignored, the consequence may be disastrous for the loss of consciousness could be abrupt and this is too late for treatment.
Attacks may differ from time to time and should never be taken lightly. Insulin is injected under the skin (subcutaneously) – not into the muscle. It is important that someone near you knows that you have used insulin and is aware of the effects and treatment of hypoglycaemia. These attacks may come on suddenly and without much warning. This is the reason why there is a need for someone close to you to know about the use of insulin and the treatment of its side effects.
Not all insulin works at the same rate. Some insulin works very quickly while others take longer before they have an effect. Not understanding how quickly each type of insulin works can be very dangerous.
Insulin Growth Factor 1
Insulin Growth Factor 1 (igf-1) is important for metabolism as it is the factor that mediates the metabolic effects of Human Growth Hormone in the body. The main source of igf-1 is the liver but it is also produced in the kidney, muscle, pituitary gland and the gastro-intestinal tract. The function of igf-1 in the muscle is to increase protein synthesis and decrease protein breakdown. It will also decrease in the fat levels of the body.
Igf-1 is manufactured by genetic engineering techniques. There is very little indication for its use in the medical field and for that reason there is no readily available medicinal product. This leads to the dissemination of counterfeit materials, which masquerade as igf-1 and flood the market with fakes at a high cost to the buyer. As a result of the manufacturing process, it is combined with an animal protein. When injected into humans, this preparation may set up an antigen antibody reaction and this can lead to allergic reactions. The most important of these is anaphylactic shock a life threatening condition which should be treated as a medical emergency. There is also a long term possibility of the body developing an antibody to its own insulin leading to diabetes, which would be very difficult to treat as the allergy may also extend to the insulin ordered for management of the diabetes.
Igf-1 is bound to protein in the plasma and this enables its action to continue for hours, unlike hgh, which is short acting. Igf-1 causes a lowering in the blood sugar levels and it is important that insulin is not used at the same time as this increases the risks involved. Also, it is important that there is an adequate intake of food nutrients to benefit from the use of igf-1. The diet must be high in carbohydrate and contain sufficient protein for cellular reproduction. A regular intake of a wide variety of foods is the best approach.
There is a degree of interaction between hgh, insulin and igf-1 and, when using any of these substances one must always take care that someone else is aware of it and knows the treatment for hypoglycaemia.
Clenbuterol
Clenbuterol is a direct-acting sympathomimetic agent and is used as a bronchodilator in the management of asthma and obstructive lung disease. It has an advantage over salbutamol in that its action is longer lasting. It has also been used to increase the development of muscle in cattle. In humans it is effective in reducing body fat, thus its attraction to the body building community. The adverse effects are those of stimulation of the sympathetic nervous system. These are a feeling of nervousness, tremor of the hands, palpitations, headache, insomnia and a rapid pulse rate. In extreme cases there have been cases of acute poisoning with this drug. If any of these symptoms develop, the drug should be stopped immediately and medical advice sought.
Creatine
Creatine is an essential step in the delivery of energy for muscle contraction. It is a major factor in the conversion of adp (adenosine tri-phosphate) into atp (adenosine di-phosphate), which is the source of energy for contraction of the muscle cell. Creatine has been isolated and is available as a supplement for training. It does not reduce the need to train at a high intensity, but makes the contraction slightly faster and enables recovery to ensue more rapidly, as there is more creatine to allow the conversion of adp to atp. It is this reaction which makes creatine useful in training.
Human Chorionic Gonadotrophin (HCG)
Human Chorionic Gonadotrophin is secreted by the pituitary gland and stimulates the formation of Luteinising Hormone (lh). Lh stimulates the Leydig cells to form testosterone. It is this action that is of interest to anabolic steroid users. During a course of steroids there is inevitably some reduction in sperm numbers due to suppression of Follicle Stimulating Hormone. The effects of the anabolic steroid upon the release of Gonadotrophin Releasing Hormone cause this from the hypothalamus. On ceasing the course of anabolic steroids the size of the testes will recover and sperm growth will return to normal providing that the course of steroid is within reasonable limits.
The practice of using hcg near the end of a course of steroids to stimulate the testes is baseless and inefficient. At the end of a steroid course, the pituitary gland slowly resumes normal function in most cases and restores the correct balance of hormones. If hcg is used, it takes over the duty of the pituitary gland in starting the recovery of the normal balance. Once hcg is ceased, the testes return to their reduced size and the pituitary resumes its recovery. The use of hcg during a course cannot be recommended, as it only slows the permanent recovery. It has also been associated with the development of gynaecomastia.
Tamoxifen
Tamoxifen (Nolvadex) is an anti-oestrogenic agent commonly prescribed for the treatment of oestrogen dependent breast tumours. Tamoxifen achieves this effect by binding to the target receptor sites. Tamoxifen is used by anabolic steroid users to prevent or reduce gynaecomastia, caused by aromatisation or when endogenous testosterone levels are suppressed.
Diuretics
Diuretics are used by athletes to lose weight and, at times, the bloated look of water retention due to anabolic steroid use. They all have the same basic result, in that they cause the body to lose water. However the individual drugs do this by different mechanisms. Some diuretics lead to the excretion of larger amounts of electrolytes than others. It has been known for individuals to take potassium supplements to try and replace this electrolyte.
Potassium supplementation is potentially dangerous and has been associated with cardiac arrest.
Testosterone Precursors
There are a number of products in this category that are very similar in their actions. They are all part of the metabolic chain leading to the development of testosterone. The first of these is dehydroepiandrosterone (dhea), closely followed by Androstenedione and Androstenediol. The first two of these are also made by the adrenal gland in its normal function they contribute less than 5% of the total daily production of testosterone. When present, dhea and Androstenedione are converted to testosterone or oestrone. Androstenediol can only be converted to testosterone. For those who use these substances it can be expected that they will act like anabolic steroids and produce similar results. It is essential that these drugs produce testosterone and its life in the serum is very short and any effects are likely to be minimal. Research suggests that the results obtained with these substances are no better than hard training and adequate diet.
On 1 September 1996 anabolic steroids and a number of related substances became subject to the controls of the Misuse of Drugs Act. The
controls are not as strict as for drugs such as heroin and are aimed more at the dealer than the user. Prior to the change in legislation, steroids came under the jurisdiction of the Medicines Control Agency, an arm of the Department of Health.
Anabolic steroids, Growth Hormone (HGH), Clenbuterol and Human Chorionic Gonadotrophin (HCG) all became Class C drugs under the Misuse of Drugs Act 1971. The maximum penalties available for offences involving Class C drugs are currently 5 years imprisonment or an unlimited fine, or both.
What does all this mean to the man in the street? It is now an offence to supply any of the above mentioned anabolic substances without a Home Office licence (‘supply’ is not restricted to selling these drugs, but includes giving to, lending to and sharing them with other people).
However, simple possession of an anabolic substance, when in the form of a medicinal product, is not an offence, although possession with intent to supply is an offence. This is a grey area and there are no hard and fast guidelines as to what sort of amount the police would consider a ‘dealer quantity’. Even a few ampoules might be, if, for example, you had been supplying them earlier.
Section 4: Drug Profiles

The following section contains details of some of the most commonly used anabolic steroids and associated performance enhancing drugs. The ‘Street Info’ is a summary of some of the commonly held beliefs and views of steroid users regarding these drugs.
Administration
Injectable
Alternative Names
Boldenone Undecylenate
Veterinary Products
Boldebal-H (50mg/ml), Equipoise (25, 50mg/ml), Ganabol (25, 50mg/ml), Pace (50mg/ml), Sybolin (25mg/ml), Vebonol (25mg/ml).
The Lowdown
Boldenone undecenoate is an oil based anabolic steroid used in veterinary practice. Drive contains Boldenone undecenoate in addition to Methandriol Dipropionate.
Street Info
Equipoise is commonly thought to be effective in producing rapid increases in strength and muscle mass and has also been used for ‘cutting’ prior to competition.
Nandrolone Decanoate
Administration
Injectable
Alternative Names
Nortestosterone Decanoate, Nortestosterone Decylate
Proprietary Names
Anaboline (50mg/ml), Anabolin LA-100Deca-Durabol (25, 50,
100mg/ml), Deca-Durabolin (25, 50, 100, 200mg/ml), Dece-ject (25, 50mg/ml), Elpihormo (50mg/ml), Extraboline (50mg/ml), Hybolin Decanoate (50, 100mg/ml), Jebolan (50mg/ml), Nandrolone Decanoate (50,100, 200mg/ml), Nurezan (50mg/ml), Retabolil (25, 50mg/ml), Retabolin (50mg/ml), Turinabol Depot (50mg/ml), Ziremilon (50mg/ml).
Vetinary Products
Anabolicum, Norandren.
Nandrolone Decanoate in the form of the Organon product, Deca- Durabolin has been around for over thirty years.
As Nandrolone is not C17 alpha-alkylated it does not have as strong an association with the occurrence of liver dysfunction and cholestasis. However, it may cause fluid retention and oedema due to sodium retention by the kidney.
Street Info
Nandrolone Decanoate (Deca) is widely considered to be the most commonly used injectable anabolic steroid used for performance enhancement. It also has the reputation for being one of the most frequently detected banned substances (metabolites can be detected for periods in excess of one year). Because of its popularity Deca has been widely counterfeited. Due to its relatively low androgenic properties it is also commonly thought to aromatise only at high doses. Deca is commonly used for ‘bulking-up’ and has a reputation for promoting size and strength.
Reports of side effects include hypertension, acne, sexual and reproductive problems. The occurrence of side effects appear to be more common in females and are influenced strongly by the dosage used.
Methandrostenolone
Administration
Oral
Alternative Names
Methandienon
Proprietary Names
Anabol (5mg), Andoredan (5mg), Bionabol (2, 5mg), Encephan (5mg), Metabol (5mg), Metaboline (5mg) also contains multivitamins and nutrients, Metanabol (1, 5mg), Methandrostenolonum (5mg), Naposim (5mg), Nerobol (5mg), Pronabol (5mg), Stenolon(1, 5mg),Trinergic (5mg capsules).
Vetinary/Injectable 25mg/ml.
Anabolikum, Metandiabol.
The Low Down
Methandrostenolone usually referred to as Dianabol was first produced and marketted by Ciba-Geigy in 1960. It was promoted as being highly anabolic. Dianabol was also reported to enhance feelings of well being.
Methandrostenolone and Methandienone are almost identical, the only difference being in the spatial configuration of their chemical structure. They are C-17 alpha-alkylated compounds and therefore exert a significant strain on the liver, with even relatively low dosages causing temporary abnormalities in liver function tests.
Street Info
Many users of this steroid have reported dramatic gains in both strength and size. However, it aromatises even at low dosages, with the development of gynaecomastia a common problem. Another common complaint is the problem of water retention, resulting in hypertension.
Female use of Methandrostenolone/Methandienone can result in virilisation due to its androgenic properties. Masculinising effects can occur even at low dosages in some women who are particularly sensitive to androgens.
Oxandrolone
Administration
Oral
Proprietary Names
Anavar (2.5mg), Lipidex (2.5mg), Lonavar (2mg), Oxandrin (2.5mg), Vasorome (2.5mg).
The Lowdown
Oxandrolone is C-17 alpha-alkylated so there is the potential for liver damage.
Street Info
Oxandrolone has relatively low androgenic properties, with little aromatisation in males. It has a reputation for increasing strength but not size. It is popular with women because of its low incidence of side effects due to virilisation, however some cases of facial hair growth and deepening of the voice have been reported following prolonged dosages. Gastrointestinal irritation, including pain and diarrhoea are commonly reported side effects in both male and female users.
Oxymetholone
Administration
Oral
Proprietary Names
Adroyd (50mg), Anadrol 50 (50mg), Anapolon (5mg), Anapalon 50 (50mg) Hemogenin (50mg), Oxitosona (50mg), Plenastril (50mg), Roborol (50mg), Synasteron (50mg).
The Lowdown
Oxymetholone is C-17 alpha-alkylated, with liver disturbances and jaundice common even at therapeutic doses. There have also been links between Oxymetholone treatment and the development of leukaemia.
Street Info
Oxymetholone, a derivative of dihydrotestosterone (DHT) and is commonly recognised as the strongest oral anabolic steroid available. It is both highly anabolic and androgenic and being
C-17 alpha-alkylated, very toxic to the liver. There have been many reports of acne and hair loss (due to high levels of DHT) in addition to its strong association with liver damage and gynaecomastia. There have also been reports of headaches and stomach pains. There is substantial evidence of loss of size and weight, which has been attributed to the drug being too hard on the body. Very few women are able to tolerate oxymetholone due to its virilising effects.
Stanozolol
Administration
Oral
Alternative Names
Androstanazole, Methylstanazole
Proprietary Names
Stromba (5mg), Winstrol (2mg).
The Lowdown
Stanozolol, when given for prolonged periods, has been associated with elevated liver function results due to the fact that it is a
C-17 alpha-alkylated compound.
Street Info
Stanozolol tablets have a reputation for causing gastrointestinal discomfort after prolonged use. Both the tablets and injection form are not considered to aromatise. Tablets are often taken in divided doses to reduce the gastric irritation. This practice is popular with female users, as it reduces the risks of virilisation which is associated with large amounts of androgens in the female system.
Sustanon 250
Administration
Injectable
Proprietary Names
Sostenon 250, Sustenon 250.
Vetinary Products
Deposterone
Make Up
Sustanon contains four different testosterones:
Testosterone Propionate 30MG Testosterone Phenylpriopionate 60MG Testosterone Isocaproate 60MG
Testosterone Decanoate 100MG
The Lowdown
Sustanon 250 has considerable anabolic and androgenic properties. It was designed to maximise the synergistic effect of using four testosterones. The variation in half-life times of the testosterones means that the product is fast acting and then remains effective for several weeks.
Street Info
Sustanon 250 has a reputation for being very effective at increasing both size and strength. The adverse effects of water retention and aromatisation leading to gynaecomastia are considered to be less pronounced than in long-acting testosterone injections.
Testosterone Enanthate
Administration
Injectable
Alternative Names
Testosterone Enantate, Testosterone Heptanoate
Proprietary Names
Androtardyl (250mg/ml), Delatestryl (200mg/ml), Durathate (200mg/ml),Malogen (100, 200mg/ml), Primoteston Depot (100, 180mg/ml), Testo-Enant (100, 250mg/ml), Testosteron Depot (50, 100, 250mg/ml), Testoviron Depot (100, 250mg/ml).
Veterinary
Testosterona 200 (200mg/ml.10ml vial)
Street Info
Testosterone Enanthate is considered to be very similar to Testosterone Cypionate but less likely to cause water retention.
Testosterone Cypionate
Administration
Injectable
Alternative Names
Testosterone Cipionate, Testosterone Cyclopentylpropionate
Proprietary Names
Andro-Cyp (100, 200mg/ml), Depo-Testosterone (50, 100, 200mg/ ml), Depotest (100, 200mg/ml), Duratest (100, 200mg/ml), Testa-C (200mg/ml), Testex Leo (100, 250mg/2ml)
The Lowdown
Testosterone Cypionate is an ester of testosterone with high anabolic and androgenic properties. It is oil based and therefore long acting.
Street Info
Testosterone Cypionate is considered to aromatise easily leading to problems such as gynaecomastia. Large dosages have been associated with causing psychological effects including aggression. Hypertension, acne and premature balding are also commonly reported problems.
Methenolone Acetate
Administration
Oral
Alternative Names
Metenolone Acetate
Proprietary Names
Primobolan (5mg), Primobolan S (25mg)
The Lowdown
Primobolan tablets are not C-17 alpha-alkylated and do not have the liver toxicity associated with many of the other oral anabolic steroids.
Street Info
Primobolan has a reputation for having low androgenic properties causing little aromatisation, water retention or liver damage. It is generally considered to be one of the safest anabolic steroids. Muscle gains are reported to be slow to develop but of good quality.
Counterfeits and Fakes
The existence of counterfeit anabolic steroids is by no means a new phenomenon. Due to the limited availability of genuine pharmaceutical products and the laws of supply and demand, many anabolic steroid users have grown to accept the fact that the majority of products available to them will be either fake or counterfeit. However it is important to note that although the terms fake and counterfeit may imply inferior quality, there is evidence to suggest that many of these products do in fact contain anabolic steroids (although not always of the dosage or type specified). In some instances these products have acquired such a positive reputation that they have become sought after in their own right, even to the extent of being counterfeited themselves.
Traditionally, fake anabolic steroids were relatively easy to identify. Poor packaging, badly printed or photocopied
information inserts and bar codes that often appeared to have been drawn with a felt tip pen were and still are the most obvious indications of fake products. Other pointers include visible contamination of ampoules, variability in appearance and content of ampoules and vials, and incorrect tablet consistency. There are, however, exceptions to these guidelines as is evident in the poor quality packaging of genuine pharmaceutical products manufactured in developing countries. While it is still possible to find these rather amateurish fakes being sold to the unwary, a more sophisticated type of product has appeared on the market which is much more difficult to identify.
One of the most disturbing aspects of fake and counterfeit anabolic steroids is the variations in content of these products. This is especially significant when one considers that some anabolic steroids which have been tested were found to contain nearly twice the strength of the stated content. These results clearly demonstrate the problems facing anabolic steroid users who purchase products on the illicit market. Many users will be aware of the probability of a product being fake or counterfeit. There is often the presumption that the fake steroid will be weaker than the stated content. The user will often compensate for this by increasing the amount taken. As illustrated above this could be a very dangerous practice.
In addition to the strength variations of illicitly produced anabolic steroids, there are many examples of the stated anabolic steroid being substituted with a different active ingredient. There have been cases of high androgenic anabolic steroids being packaged as steroids with much lower androgenic properties. Many of the side effects associated with anabolic steroids are a direct result of their androgenic properties. The potential for harm can be greatly increased if large doses of high androgenic anabolic steroids are used. The risk to female anabolic steroid users is particularly worrying as the virilising effect of androgens in women can result in irreversible side effects.
 Section 5: Intramuscular Injections for Anabolic Steroids
Section 5: Intramuscular Injections for Anabolic Steroids
Injecting drugs can be a hazardous procedure with serious risk of injury and disease. Anabolic steroid injectors need to follow some basic rules and procedures to minimise the potential harm. Thankfully, most risks are easily avoided by following a few basic rules and procedures.
Anabolic Steroids should only be injected into a muscle and the following pages provide basic instruction on intramuscular injection. Anyone considering self-injection should first get advice from a health professional. Prospective injectors should approach their doctor or go to a needle exchange service or a local drugs agency.
“Anabolic steroid injectors need to follow some basic rules and procedures to minimise the potential harm”
1

Sterile Equipment
A clean needle and syringe should be used for each injection. By ‘clean’ we mean equipment which has just been removed from its sealed wrapper. No injecting equipment should be shared with anybody else under any circumstances. Sterile injecting equipment and boxes for the safe disposal of contaminated sharps can be obtained from your local syringe exchange.
The Correct Equipment
Not just any needle will do. The needle must be long enough to reach into the muscle and of a sufficient bore to enable an oil based solution to be injected with the minimum of tissue damage. For an intramuscular injection to be given correctly, either a 21g x 1.5” (long green) or a 23g x 1.25” (long blue) needle is usually required. Two needles are needed for each injection – one to draw up with and one to inject. A 2ml syringe should be used as this is the maximum volume that should be injected into a muscle at any one time.
Keep it Clean


Gather together all the sterile equipment for the injection on a clean and clear surface. Remember, no equipment whatsoever should be shared.
![]()
Before proceeding, hands and the part of the body to be injected should be washed thoroughly with hot water and soap. By piercing the skin with a needle the injector is opening the door for bacteria. Keeping clean is vital to avoid infection. Using a sterile alcohol swab will help but it is not a substitute for soap and water.
![]()
2
Drawing Up From An Ampoule or Vial

Before drawing up a solution it should be examined for any signs of contamination. If there are any particles visible, if the seal is broken or if the solution is discoloured, it should not be used.
![]()
Allow solutions that have been refrigerated to reach room temperature before injection.
![]()
When drawing up a solution into a syringe the needle may become blunt as it passes through the rubber seal on the top of a vial, or if it is scraped against the inside of an ampoule. If a blunt needle is used to inject it may damage the muscle and can cause pain. The solution should be drawn up slowly and the used needle disposed of into a ‘contaminated sharps’ box and replaced with a new one.
![]()
Any air bubbles should be expelled by holding the syringe upwards and flicking the barrel. The plunger is then pressed until a drop of the solution appears at the tip of the needle.
4
Where to Inject
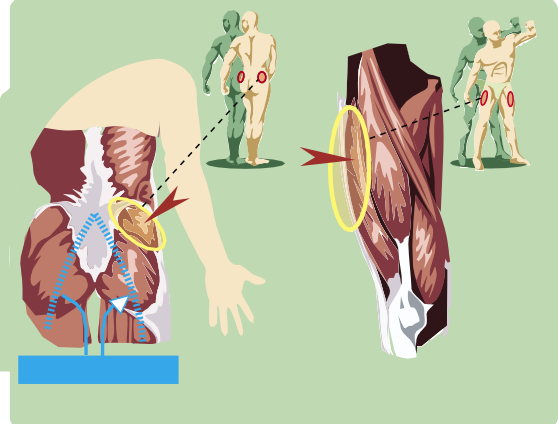
SCIATIC NERVES
A health professional or good gym instructor will be able to show you the exact location of the gluteus maximus and vastus lateralis muscles on your body.
The blue lines indicate the likely pathway of the sciatic nerves – hitting these when injecting is very painful and can also be very dangerous.
Anabolic steriods should never be injected into a vein. They should only ever be injected into a muscle. The main sites for intramuscular injections are the upper outer quadrant of the buttock (Gluteus maximus) and the middle outer muscle of the thigh (Vastus lateralis). Since the pathway of the sciatic nerves is around the Gluteus maximus, it is important to inject carefully in this area. Hitting the sciatic nerves is very painful and can be very dangerous.
Injection sites should be rotated for successive injections to avoid too much damage in any one place. Since steriods work throughout the body and not locally, it is pointless to target particular muscle groups with injections.
Other Sites
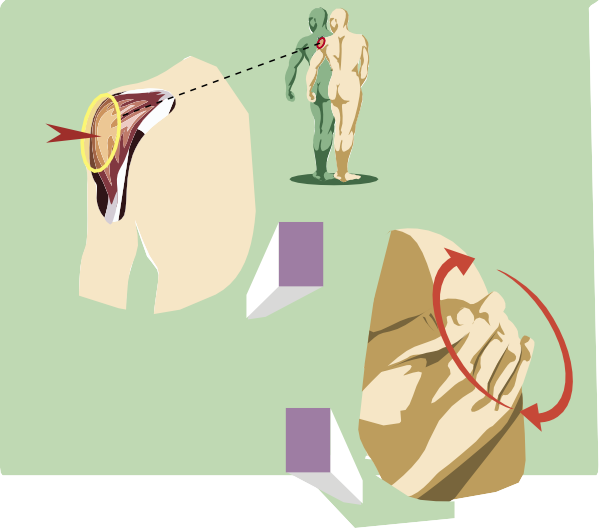
If it is not possible to inject into the thighs or buttocks, the deltoids are the next best site for intramuscular injection.
![]()
The smaller the muscle, the more pain and damage an injection will cause. Great care should be taken. Warm oil-based solutions to body temperature, inject slowly and then gently massage the area to help distribute the drug.
![]()
5
Pre-injection
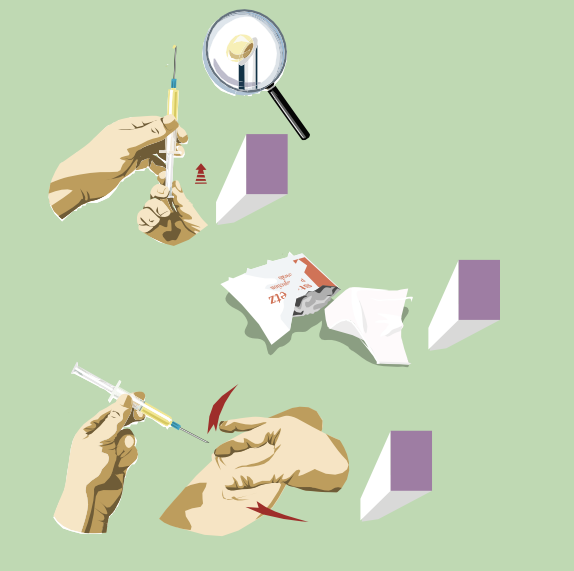
Get rid of any air bubbles in the syringe. Flick the barrel to send them to the top of the syringe and then press the plunger until a drop appears at the tip of the needle.
![]()
If you use an alcohol swab on the injection site, allow a few seconds for your skin to dry before using the needle. There is no reason to use a swab if your skin is clean. Soap and water is a healthier option.
![]()
Use your thumb and forefinger to stretch out the bit of skin where you are going to inject.
![]()
6
The Injection

With the syringe held like a dart, the needle is pushed through the skin and into the muscle. There is no need to insert the needle to the hilt and care should be taken to avoid hitting bone.
![]()
Before injecting the solution it is necessary to check the needle is not in a blood vessel. The plunger is eased back to make sure no blood is seen in the syringe. If blood appears, then the needle must be removed and the injection reattempted.
![]()
To minimise damage, it is important that the solution be injected slowly.
![]()
7
Post-injection

A small amount of bleeding at the injection site is normal. Direct pressure applied with a clean tissue for a few minutes will stop the bleeding and help prevent bruising. Other transient effects include slight swelling, redness, burning, or itching. These should subside shortly.
![]()
Used needles, syringes, swabs and empty ampoules should be placed in a ‘contaminated sharps’ container and returned to an agency operating a syringe exchange scheme for safe disposal.
![]()
Remember to wash your hands thoroughly.
![]()
8
Complications of Poor Injecting Techniques
Infection
Sharing of injecting equipment can lead to many infections including Hepatitis B and HIV. Poor hygiene or unsterile equipment can cause inflammation or abscesses at the injection site which may be hard to heal.
Nerve, Tendon and Ligament Damage
Incorrect siting of injections can cause damage to tendons and ligaments causing pain and impairing training. Severe nerve damage can occur resulting in impaired sensation or even paralysis. This may result in long term mobility problems.
Muscle Damage
Repeated injections into the same muscle group can cause destruction and breakdown of the muscle tissue, resulting in impaired muscle function. Any subsequent injections in the damaged muscle will be both painful and poorly absorbed in the scarred tissue.
Haemorrhage
Accidental puncture of a blood vessel inside the muscle can cause bleeding and the formation of bruising deep inside the muscle. This may result in stiffness and discomfort, restricting training ability and performance.
Text by Pat Lenehan and Tony Miller Design and Illustration by Richard Kemplay
© Lifeline Publications 2004. All rights reserved.
![]() aims
aims
To provide detailed information on
Anabolic steroid use and substances. This booklet also includes a step- by-step guide to intra-muscular injection, the purpose of which is to encourage safer practise.
audience
![]()
Drug workers and anabolic steroid
users, aged 18+
content
Some illustrations of drug use, no swearing funding
Self-financed
39-41 Thomas Street | Manchester M4 1NA | lifeline is a registered charity no: 515691
+44 (0) 161 839 2075 | www.lifelinepublications.org.uk | [email protected]
lifeline publications